
Inflammation — MCQs

On this page
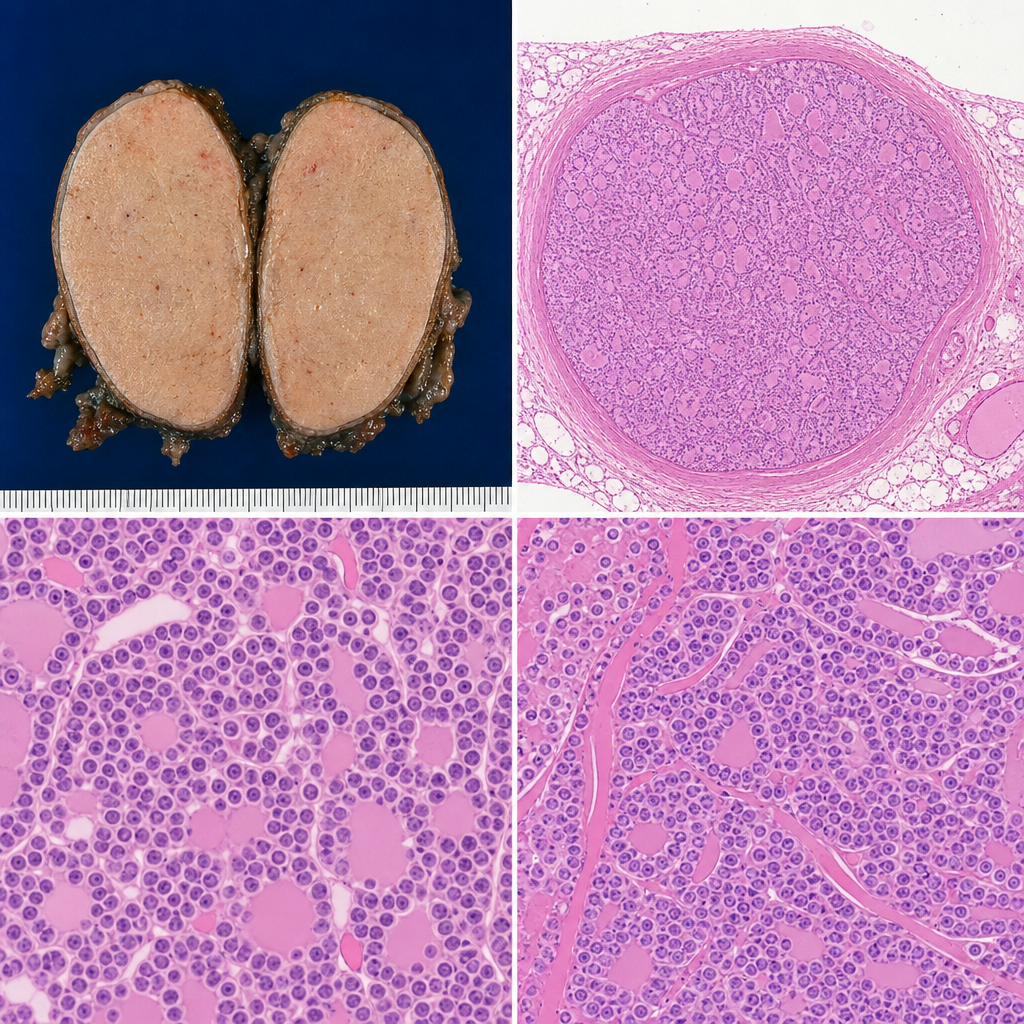
A 34-year-old woman presents with a painless neck mass that has been enlarging for 3 months. Fine-needle aspiration is performed. The aspirate shows cohesive clusters of follicular cells arranged in microfollicular and trabecular patterns. The nuclei are round to oval with evenly distributed chromatin, smooth nuclear membranes, and no grooves or intranuclear inclusions. No psammoma bodies are identified. A well-encapsulated follicular neoplasm is subsequently resected. Which of the following additional histological features would most reliably confirm malignancy in this lesion rather than indicating a benign follicular adenoma?
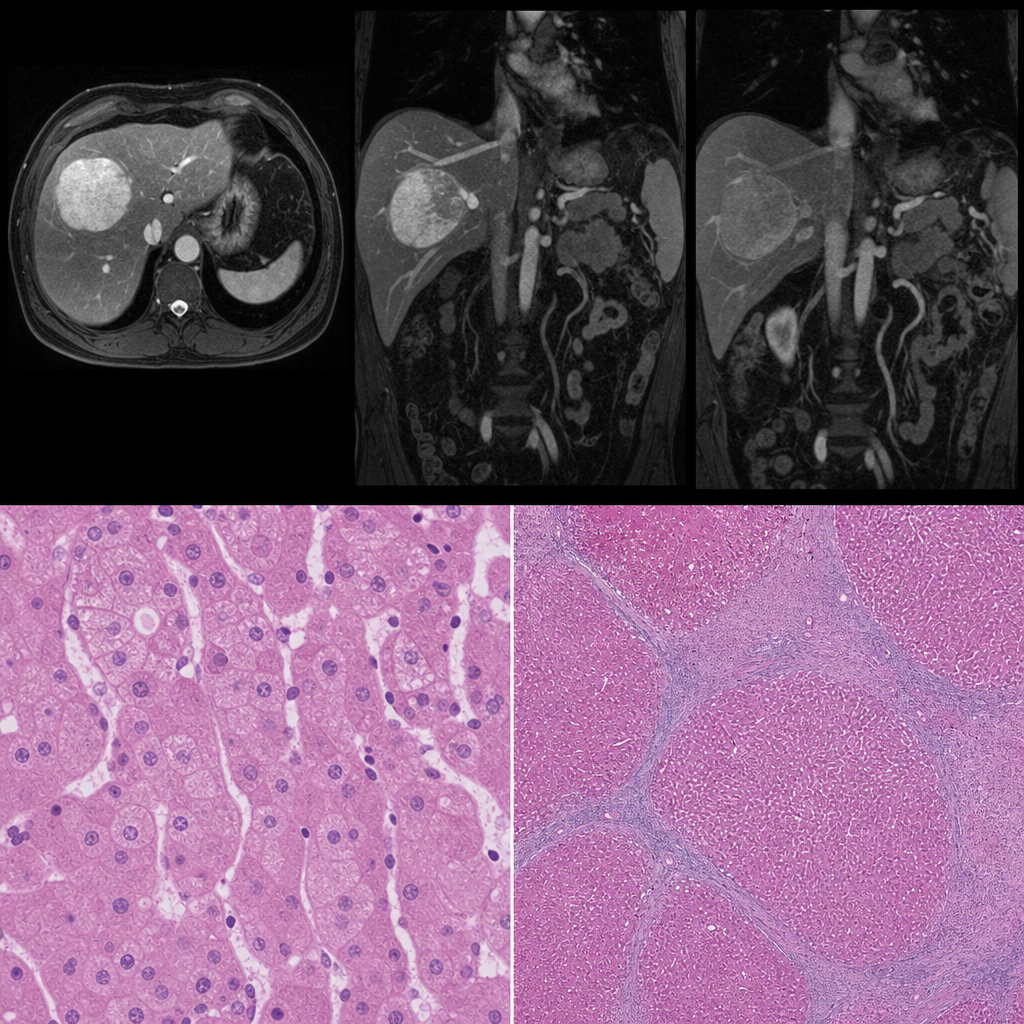
A 67-year-old man with a 30-year history of alcohol use disorder presents with jaundice, ascites, and a serum AFP of 620 ng/mL. Abdominal MRI shows a 5 cm arterially enhancing hepatic mass with washout on portal venous phase. A liver biopsy from the mass is performed. The photomicrograph shows trabeculae of large polygonal cells with abundant granular eosinophilic cytoplasm, prominent nucleoli, and intracytoplasmic hyaline globules; adjacent non-tumoral liver shows bridging fibrosis and regenerative nodules. Mallory-Denk bodies are identified in some tumor cells. Which of the following findings, if present, would most specifically distinguish this lesion from a benign hepatocellular adenoma in this biopsy?
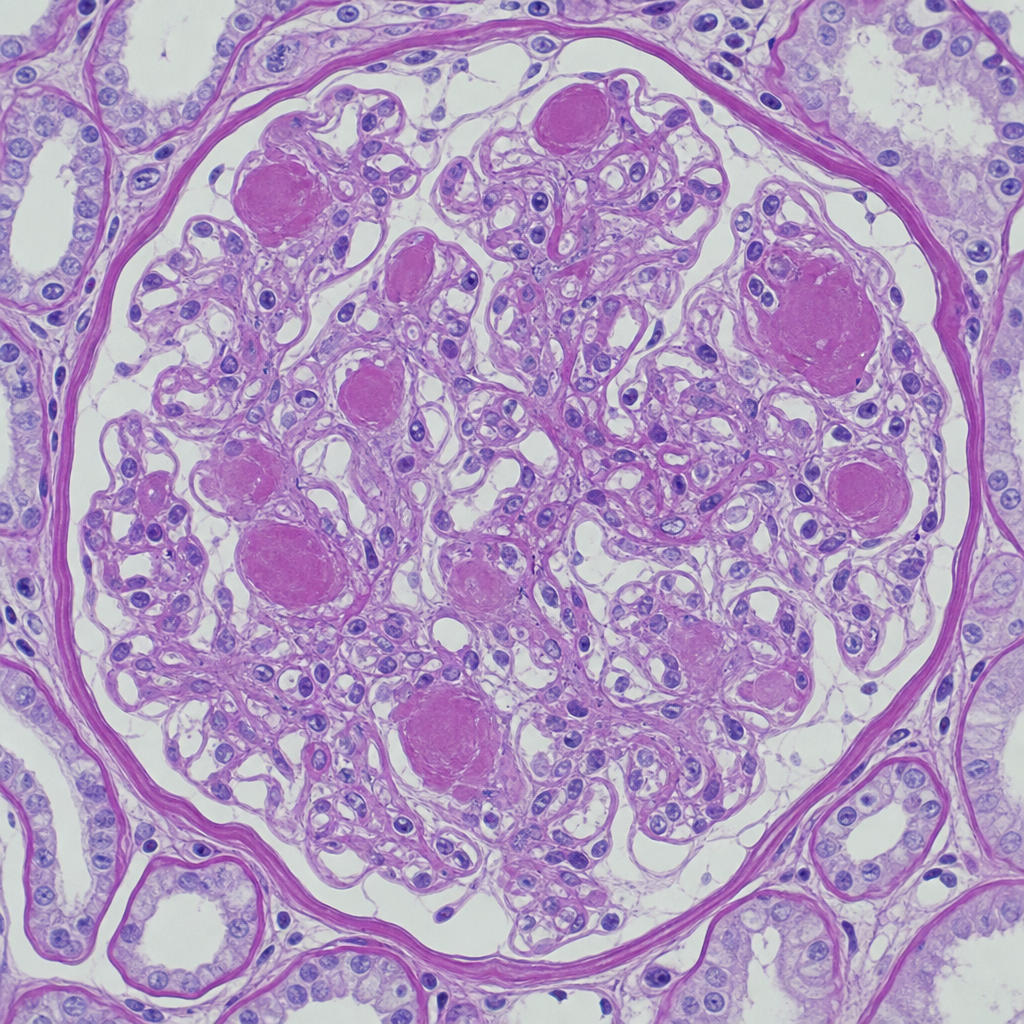
A 67-year-old man with longstanding poorly controlled type 2 diabetes mellitus and hypertension undergoes renal biopsy for nephrotic-range proteinuria and progressive renal insufficiency. He is also known to have longstanding diabetic retinopathy, and immunofluorescence staining for monoclonal light chains is negative. The photomicrograph of a PAS-stained section shows glomeruli with expanded mesangium containing ovoid, homogeneous, PAS-positive nodular deposits situated at the periphery of the glomerular tuft, compressing the adjacent capillary loops. The deposits stain negatively with Congo red. Which of the following best describes the composition and pathogenesis of these nodular deposits?
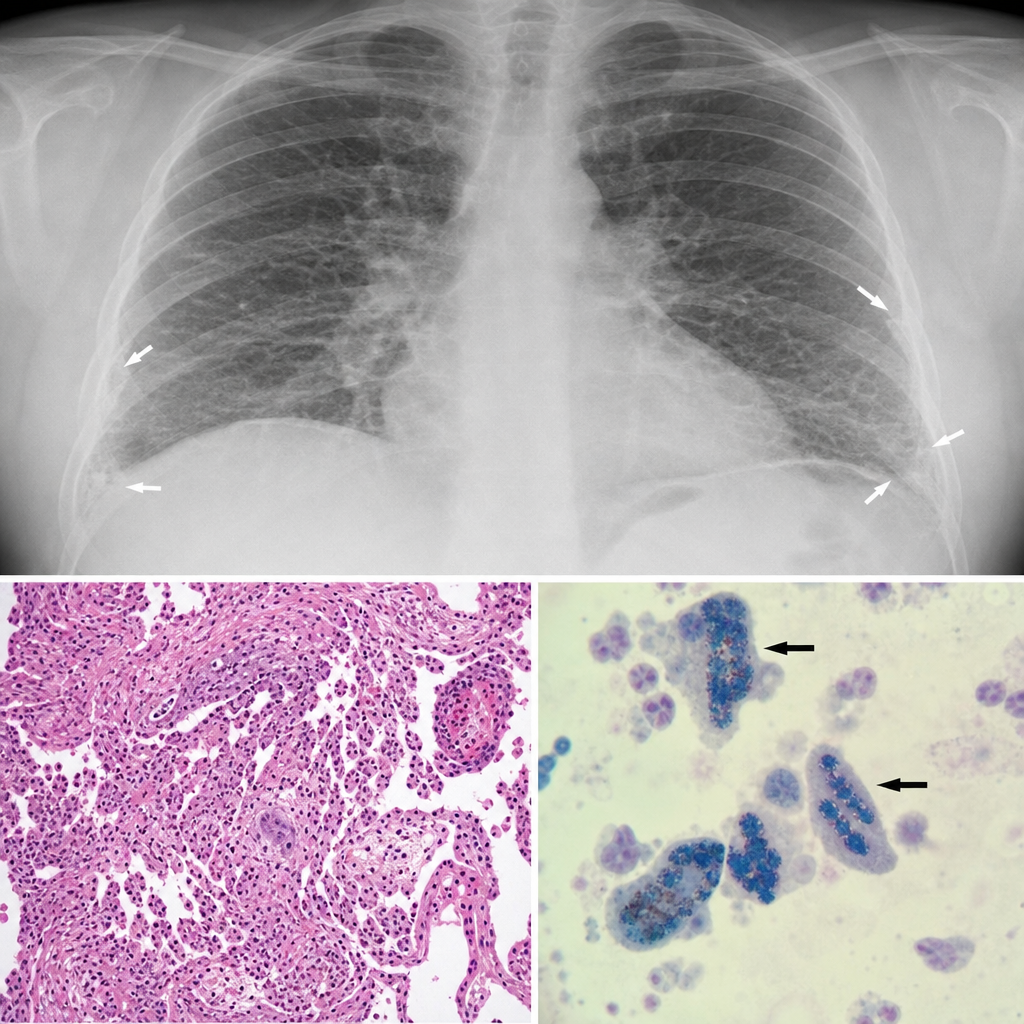
A 58-year-old man presents with progressive exertional dyspnea and a dry cough over 8 months. He worked in shipbuilding for 25 years. A chest radiograph shows bilateral lower-lobe reticular opacities and pleural plaques. A transbronchial biopsy is performed. The biopsy reveals dense interstitial fibrosis with golden-brown, beaded, dumbbell-shaped structures within alveolar macrophages that stain positively with Prussian blue. Which of the following best describes the pathological significance of the structures identified in this biopsy?
A 42-year-old man who recently immigrated from Mexico presents to the clinic with fever, a productive cough streaked with blood, back pain, and night sweats. He was found to be HIV-positive 3 years ago but does not know his most recent CD4+ count. With further questioning, the patient notes that he had previously experienced these symptoms when he was in Mexico, but he has no recollection of taking any treatment. Which of the following characteristics would best describe the histology of a lung biopsy specimen obtained from this patient?
A 48-year-old man comes to the physician because of a 2-day history of fever, flank pain, and hematuria. He has chronic back pain, for which he has been taking meloxicam for the past 2 weeks. His temperature is 38.9°C (102°F). Physical examination shows a diffuse maculopapular rash over his trunk and extremities. Urinalysis shows 10–15 RBC/hpf, 20 WBC/hpf, and numerous eosinophils. Histologic examination of a kidney biopsy specimen is most likely to show which of the following findings?
A 3-year-old boy is brought to the physician for follow-up examination 5 days after sustaining a forehead laceration. Examination shows a linear, well-approximated laceration over the right temple. The wound is clean and dry with no exudate. There is a small amount of pink granulation tissue present. Microscopic examination of the wound is most likely to show which of the following?
A 9-year-old boy is brought to the hospital by his mother with complaints of fever and right flank pain for the past 3 days. His mom mentions that he has had these symptoms recurrently for the past 4 years. He was treated with antibiotics in the past and got better, but eventually, these symptoms recurred. On physical examination, he is warm to touch and there is tenderness over his right costovertebral angle. The vital signs include a blood pressure of 100/64 mm Hg, a pulse of 100/min, a temperature of 38.0°C (100.4°F), and a respiratory rate of 14/min. Complete blood count results are as follows: Hemoglobin 12 g/dL Red blood cell 5.1 million cells/µL Hematocrit 45% Total leukocyte count 8,500 cells/µL Neutrophils 71% Lymphocyte 24% Monocytes 4% Eosinophil 1% Basophils 0% Platelets 240,000 cells/µL Urinalysis results: pH 6.2 Color turbid yellow RBC none WBC 8–10/HPF Protein trace Cast WBC casts Glucose absent Crystal none Ketone absent Nitrite positive A computed tomography scan shows renal scarring and multiple atrophy sites with compensatory hypertrophy of residual normal tissue. There is additional renal cortical thinning. Which of the following would be the most likely microscopic finding if a renal biopsy were to be done?
A 60-year-old man comes to the office because of an 8-month history of cough, night sweats, shortness of breath, and fatigue. He has also had a 9-kg (19.8-lb) weight loss during this time. He appears pale. Abdominal examination shows hepatosplenomegaly. His leukocyte count is 80,000/mm3 and his leukocyte alkaline phosphatase level is increased. A peripheral blood smear shows > 82% neutrophils with band forms and immature and mature neutrophil precursors. An x-ray of the chest shows a 9-mm right hilar nodule. Which of the following is the most likely cause of this patient's laboratory findings?
A 22-year-old man presents with multiple, target-like skin lesions on his right and left upper and lower limbs. He says that the lesions appeared 4 days ago and that, over the last 24 hours, they have extended to his torso. Past medical history is significant for pruritus and pain on the left border of his lower lip 1 week ago, followed by the development of an oral ulcerative lesion. On physical examination, multiple round erythematous papules with a central blister, a pale ring of edema surrounding a dark red inflammatory zone, and an erythematous halo are noted. Mucosal surfaces are free of any ulcerative and exudative lesions. Which of the following statements best explains the pathogenesis underlying this patient’s condition?
Practice by Chapter
Acute inflammation mechanisms
Practice Questions
Vascular changes in inflammation
Practice Questions
Chemical mediators of inflammation
Practice Questions
Cellular components of inflammation
Practice Questions
Resolution of acute inflammation
Practice Questions
Chronic inflammation
Practice Questions
Granulomatous inflammation
Practice Questions
Systemic effects of inflammation
Practice Questions
Patterns of inflammatory response
Practice Questions
Inflammatory markers in laboratory testing
Practice Questions
Anti-inflammatory therapies
Practice Questions
Wound healing and repair
Practice Questions
Abnormalities in wound healing
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app